Guide for hepatocyte ballooning: Causes and steatosis comparison

Metabolic dysfunction-associated steatohepatitis (MASH) is a significant public health concern. Two reasons set the alarm: an estimated global prevalence of 5.27% and a lack of approved pharmacological treatments.
Among the key histological features of this disease, hepatocyte ballooning stands out as a critical marker for diagnosing and understanding disease progression.
.
What is hepatocyte ballooning?
.
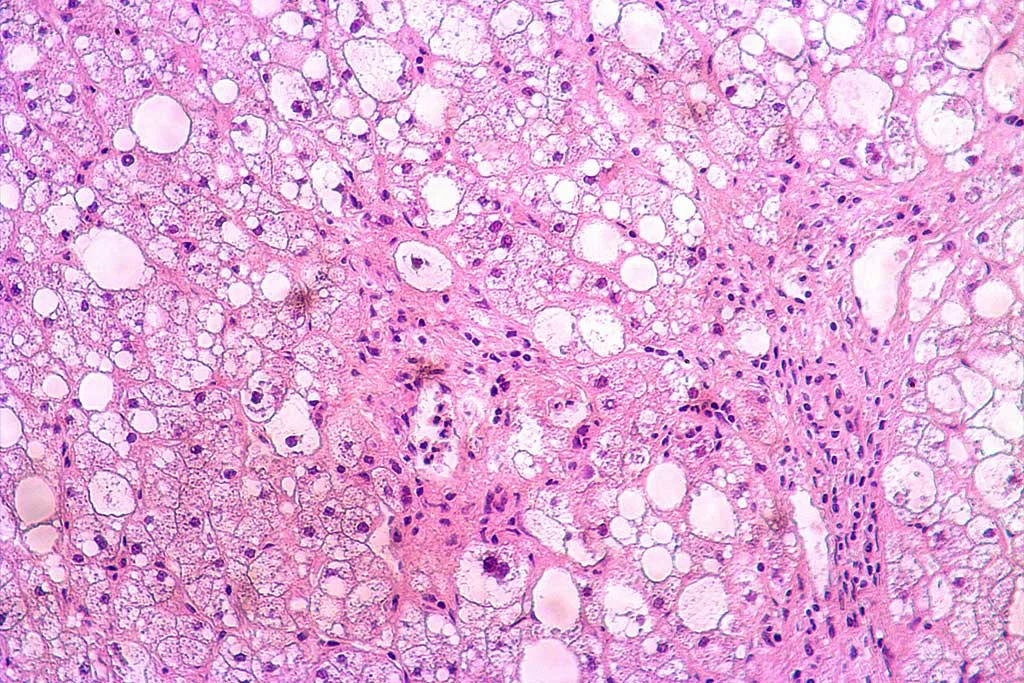
Hepatocyte ballooning refers to the abnormal swelling, enlargement, and rounding of hepatocytes characterized by a reticulated cytoplasm. When examined under the microscope, ballooned hepatocytes are typically large and round and have a diameter 1.5-2 times greater than regular hepatocytes. Hematoxylin and eosin (H&E) staining reveals a pale and eosinophilic cytoplasm, with the presence of an excess of fatty acids, cholesterol, and ceramides.
Hepatic ballooning degeneration is a hallmark feature in advanced liver diseases such as MASH. However, hepatocyte ballooning is not only commonly observed in alcoholic steatohepatitis but also in viral hepatitis, cholestatic liver diseases, and certain drug-induced liver injuries.
This condition is more than a structural anomaly—it signals significant cellular damage and often correlates with inflammation, oxidative stress, and the progression of liver fibrosis. It serves as a key diagnostic marker, if a biopsy is performed, to identify the progression from simple steatosis to MASH, reflecting a level of cellular damage and stress that goes beyond fat accumulation. Clinically, hepatocyte ballooning degeneration has been linked to more severe liver disease, like cirrhosis, and an increased likelihood of liver-related complications.
.
What causes hepatocyte swelling?
.
The progression of hepatocyte ballooning involves a complex interplay of cellular mechanisms, beginning with metabolic and environmental stressors:
1- The accumulation of free fatty acids, cholesterol, and ceramides, coupled with inflammation, initiates hepatocyte swelling. Cholesterol and ceramides can directly impair mitochondrial function by disrupting membrane integrity. Damaged mitochondria produce less ATP, which hampers the Na+/K+ pump’s ability to maintain cellular ion balance, causing water retention and swelling.
2- Accumulation of lipids also places stress on the endoplasmic reticulum (ER), which is responsible for protein folding and trafficking. ER stress disrupts normal protein synthesis and activates the unfolded protein response (UPR), which aims to restore cellular homeostasis but can exacerbate damage when prolonged. It increases heat shock proteins (HSPs) levels and eventually forms Mallory-Denk bodies (MDBs) as cytoskeletal damage progresses.
3- Further, sonic hedgehog (SHh) signaling becomes upregulated in response to ER stress, activating hepatic stellate cells (HSCs) and promoting fibrosis.
This sequence highlights the multifaceted nature of hepatic ballooning degeneration and its role in advancing liver disease.
.
What is the difference between steatosis and ballooning?
.
Steatosis refers to the accumulation of fatty acids in the form of triglycerides in the cytoplasm of hepatocytes. Histologically large lipid vacuoles displace the nucleus to the periphery of the cells. On the other hand, ballooning degeneration is characterized by enlarged and swollen hepatocytes with granular material in the cytoplasm, which represents a collapsed cytoskeleton.
Steatosis is associated with lipid metabolism dysregulation, while ballooning goes further, involving cytoskeletal disorganization and oxidative stress, often marked by the loss of keratin-8/18 and the presence of MDBs.
Regarding clinical implications, steatosis is considered a reversible condition when the underlying cause is addressed. It may not significantly impair liver function. Nevertheless, ballooning may suggest irreversible damage or a transition to more severe stages, such as steatohepatitis or cirrhosis. Although, in some cases, especially when it is associated with steatosis, it can be reversed by changing health habits such as diet.

Histo-morphological features of steatosis and hepatocyte ballooning (yellow arrows) from liver biopsies of patients affected by MAFLD and MASH. Hematoxylin and eosin staining. Scale bars: 100 µm. Adapted from Overi D, et al. Hepatocyte Injury and Hepatic Stem Cell Niche in the Progression of Non-Alcoholic Steatohepatitis. Cells. 2020 Mar 2;9(3):590.
.
Advancing MASH research with pathological primary hepatocytes
.
Hepatocyte ballooning is a key marker for diagnosing MASH, which currently lacks approved treatments, creating an urgent need for effective therapeutic solutions. Developing in vitro models is essential to replicate the cellular and molecular mechanisms of MASH, enabling a better understanding of lipid accumulation, inflammation, and fibrosis.
The use of primary hepatocytes in these models is key, as they closely mimic the physiological behavior and metabolic functions of human liver cells. This makes them ideal for studying disease progression and testing potential drug candidates with higher translational relevance, ultimately accelerating the discovery of targeted treatments for this prevalent condition.
BeCytes grants access to primary human hepatocytes from pathologic donors characterized for steatosis, MASH, and fibrosis to generate in vitro hepatic models. Matching tissue samples from the original biospecimen are available for each hepatocyte lot in different formats: FFPE and OCT blocks, RNA later, and snap frozen.
.

.
Each sample undergoes comprehensive analysis, including detailed characterization supported by the donor’s medical record. We also include post-thawing information: number of viable cells, viability, recommended seeding density, and cell morphology. Liver-specific functions, the activities of drug transporters, and the induction of cytochrome P450 activities are monitored.
.
.
References
American Association for the Study of Liver Diseases. “Liver Pathology: Steatohepatitis.” Accessed December 3, 2024. https://www.aasld.org/liver-fellow-network/core-series/pathology-pearls/liver-pathology-steatohepatitis
Li YY, Zheng TL, Xiao SY, Wang P, Yang WJ, Jiang LL, Chen LL, Sha JC, Jin Y, Chen SD, Byrne CD, Targher G, Li JM, Zheng MH. Hepatocytic ballooning in non-alcoholic steatohepatitis: Dilemmas and future directions. Liver Int. 2023 Jun;43(6):1170-1182. doi: 10.1111/liv.15571.
Overi D, Carpino G, Franchitto A, Onori P, Gaudio E. Hepatocyte Injury and Hepatic Stem Cell Niche in the Progression of Non-Alcoholic Steatohepatitis. Cells. 2020 Mar 2;9(3):590. doi: 10.3390/cells9030590.
Singla T, Muneshwar KN, Pathade AG, Yelne S. Hepatocytic Ballooning in Non-alcoholic Steatohepatitis: Bridging the Knowledge Gap and Charting Future Avenues. Cureus. 2023 Sep 25;15(9):e45884. doi: 10.7759/cureus.45884.
Younossi ZM, Golabi P, Paik JM, Henry A, Van Dongen C, Henry L. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): a systematic review. Hepatology. 2023 Apr 1;77(4):1335-1347. doi: 10.1097/HEP.0000000000000004.
.









{kind=link}
{kind=link}
{kind=link}
{kind=link}